We've heard from a lot of self-employed or sole-proprietors who want to take advantage of the new group of one law but are having trouble finding a health plan.
(The new law took effect in Oct. and allows qualified self-employed people buy health insurance in the less expensive small group market.)
We think we have something that can help: We've added a direct link to the federal government's Healthcare.gov site. Just type in your zipcode and you'll get a list of health plans available in your county. Of course you can also contact an agent or broker directly, but this gives you another option. Here's the link to information we've posted on our site.
If you want to bypass our website and go straight to the place that let's you enter your zipcode - here you go
Tuesday, November 30, 2010
Monday, November 29, 2010
Choline and Fatty Liver
I've been writing about non-alcoholic fatty liver disorder (NAFLD) since the early days of this blog, because it's an alarmingly common disorder (roughly a quarter of Americans affected) that is typically undiagnosed. It often progresses into its more serious cousin non-alcoholic steatohepatitis (NASH), an inflammatory condition that causes liver damage and can progress to cancer. In a number of previous posts, I pinpointed excess sugar and seed oil consumption as culprits in NAFLD and NASH (1, 2, 3, 4, 5).
Chris Masterjohn recently published two very informative posts on NAFLD/NASH that add a major additional factor to the equation: choline (6, 7). Choline is an essential nutrient that's required for the transport of fat out of the liver (8). NAFLD can be caused, and cured, simply by removing or adding dietary choline, and it appears to be dominant over other dietary factors including fat, sugar and alcohol. Apparently, certain researchers have been aware of this for some time, but it hasn't entered into the mainstream consciousness.
Could that be because the richest dietary sources are liver and eggs*? Choline is also found in smaller amounts in a variety of whole animal and plant foods. Most people don't get the officially recommended amount. From a recent review article (9):
Head over to Chris's blog and read about the classic studies he unearthed. And add The Daily Lipid to your RSS reader, because there's more interesting material to come!
The Sweet Truth about Liver and Egg Yolks
Does Choline Deficiency Contribute to Fatty Liver in Humans?
* For the brave: brain is actually the richest source of choline.
Chris Masterjohn recently published two very informative posts on NAFLD/NASH that add a major additional factor to the equation: choline (6, 7). Choline is an essential nutrient that's required for the transport of fat out of the liver (8). NAFLD can be caused, and cured, simply by removing or adding dietary choline, and it appears to be dominant over other dietary factors including fat, sugar and alcohol. Apparently, certain researchers have been aware of this for some time, but it hasn't entered into the mainstream consciousness.
Could that be because the richest dietary sources are liver and eggs*? Choline is also found in smaller amounts in a variety of whole animal and plant foods. Most people don't get the officially recommended amount. From a recent review article (9):
Mean choline intakes for older children, men, women, and pregnant women are far below the adequate intake level established by the [Institute of Medicine]. Given the importance of choline in a wide range of critical functions in the human body, coupled with less-than-optimal intakes among the population, dietary guidance should be developed to encourage the intake of choline-rich foods.I've dubbed beef liver the Most Nutritious Food in the World, Nature's Multivitamin, and I'll probably invent other titles for it in the future. Add yours to the comments. Learn to love liver! I think it's an excellent food to eat on a weekly basis.
Head over to Chris's blog and read about the classic studies he unearthed. And add The Daily Lipid to your RSS reader, because there's more interesting material to come!
The Sweet Truth about Liver and Egg Yolks
Does Choline Deficiency Contribute to Fatty Liver in Humans?
* For the brave: brain is actually the richest source of choline.
Kreidler proposes health insurance rate reforms
News release issued by Washington State Insurance Commissioner today:
Insurance Commissioner Mike Kreidler is asking state lawmakers to preserve his authority to scrutinize health insurance rates, boost transparency, and to let him—for the first time—consider some insurers’ surpluses when reviewing rates.
“Some non-profit insurers have built up hundreds of millions of dollars in surpluses in recent years, while still seeking double-digit rate hikes,” said Kreidler. “I want the law changed so we can take a closer look at that, while still maintaining a vital insurance market.”
Under current law, surpluses—including investment income—cannot be taken into account when considering a company’s rate request.
Kreidler also will seek more transparency, so consumers can have a full picture on rate proposals by insurers. Today, most information included in a rate filing is not releasable to the public.
“Tens of thousands of Washingtonians who have to buy insurance on their own struggle to find and keep coverage,” said Kreidler. “We can help protect them by continuing to review rate hikes carefully. They also deserve to see how much of their insurance premium is spent on direct medical care versus administrative overhead and profit.”
Rate review: Kreidler gained the authority to review rates in the individual market in 2008, but it’s scheduled to expire after 2011. He’s proposing legislation to do away with that deadline.
Surpluses: The surplus proposal would only apply to non-profit health insurers, which account for most of the health insurance market in Washington. Also:
• Once a company amasses a surplus equal to 3 months of claims expenses, rate hikes would not be approved.
• The insurance commissioner could grant exceptions, however, if limiting the surplus or rates would pose a threat to the financial health of an insurer.
Transparency: The legislation would allow the public to see:
• What percentage of a specific rate request goes to profit, medical costs and administrative costs.
• How much, overall, a health carrier collected in premiums, how much money it made, and how much it paid out in direct medical claims.
• The medical trends the health carrier is using to project future rates.
“It’s simple: We need oversight of the health insurance industry,” said Kreidler. “And families deserve to see where their money’s going and how their rates are set.”
Insurance Commissioner Mike Kreidler is asking state lawmakers to preserve his authority to scrutinize health insurance rates, boost transparency, and to let him—for the first time—consider some insurers’ surpluses when reviewing rates.
“Some non-profit insurers have built up hundreds of millions of dollars in surpluses in recent years, while still seeking double-digit rate hikes,” said Kreidler. “I want the law changed so we can take a closer look at that, while still maintaining a vital insurance market.”
Under current law, surpluses—including investment income—cannot be taken into account when considering a company’s rate request.
Kreidler also will seek more transparency, so consumers can have a full picture on rate proposals by insurers. Today, most information included in a rate filing is not releasable to the public.
“Tens of thousands of Washingtonians who have to buy insurance on their own struggle to find and keep coverage,” said Kreidler. “We can help protect them by continuing to review rate hikes carefully. They also deserve to see how much of their insurance premium is spent on direct medical care versus administrative overhead and profit.”
Rate review: Kreidler gained the authority to review rates in the individual market in 2008, but it’s scheduled to expire after 2011. He’s proposing legislation to do away with that deadline.
Surpluses: The surplus proposal would only apply to non-profit health insurers, which account for most of the health insurance market in Washington. Also:
• Once a company amasses a surplus equal to 3 months of claims expenses, rate hikes would not be approved.
• The insurance commissioner could grant exceptions, however, if limiting the surplus or rates would pose a threat to the financial health of an insurer.
Transparency: The legislation would allow the public to see:
• What percentage of a specific rate request goes to profit, medical costs and administrative costs.
• How much, overall, a health carrier collected in premiums, how much money it made, and how much it paid out in direct medical claims.
• The medical trends the health carrier is using to project future rates.
“It’s simple: We need oversight of the health insurance industry,” said Kreidler. “And families deserve to see where their money’s going and how their rates are set.”
Sunday, November 28, 2010
HealthCorrelator for Excel 1.0 (HCE): Call for beta testers
This call is closed. Beta testing has been successfully completed. HealthCorrelator for Excel (HCE) is now publicly available for download and use on a free trial basis. For those users who decide to buy it after trying, licenses are available for individuals and organizations.
To download a free trial version – as well as get the User Manual, view demo YouTube videos, and download and try sample datasets – visit the HealthCorrelator.com web site.
To download a free trial version – as well as get the User Manual, view demo YouTube videos, and download and try sample datasets – visit the HealthCorrelator.com web site.
Wednesday, November 24, 2010
The "Green" Agenda in Contemporary Brazil: Fact or Fiction?
 The October 2010 elections in Brazil revealed the unexpected popularity of Marina Silva, a presidential candidate supported by the small Green Party. Due to the huge size of the country, its deep heterogeneity, the comprehensiveness of the process and the absence of any mandatory linkage between regional and national representatives, the 20 million votes received by Marina Silva as a president candidate did not translate to the Green Party’s overall performance. The Green Party was and is a small party, with a modest number of representatives in the Congress (15/513), without a single senator (0/81) or governor (0/27) elected in this round.
The October 2010 elections in Brazil revealed the unexpected popularity of Marina Silva, a presidential candidate supported by the small Green Party. Due to the huge size of the country, its deep heterogeneity, the comprehensiveness of the process and the absence of any mandatory linkage between regional and national representatives, the 20 million votes received by Marina Silva as a president candidate did not translate to the Green Party’s overall performance. The Green Party was and is a small party, with a modest number of representatives in the Congress (15/513), without a single senator (0/81) or governor (0/27) elected in this round.Brazilian campaigns are relatively small and cheap compared to their North American counterparts; partially due to the fact political parties have free time on both television and radio. Nevertheless, the scope and the costs of Brazilian campaigns have been increasing, due to an increasing population (~185 million people) living in a network of over 5,500 municipalities, as well as its increasing professionalization (e.g. involving political advisors, parties’ sponsored polls etc.). Big politics is translated, in Brazil as anywhere else, into rising costs and the need to use nationwide party structures. Half of the expenses of Marina Silva’s campaign were paid by the then vice-president candidate, Guilherme Leal, founder and chairman of Natura, the world’s largest company in the field of organic cosmetics.
Marina Silva’s 20 million votes should be viewed as resulting more from a combination of her personal leadership and the growing power of Brazilian companies committed to sustainable development than to a “green boom”. In the context of a harsh competition between the two major political coalitions (supporting the elected president Dilma Rousseff and her main adversary, Jose Serra), Marina Silva also appeared to be viewed as a new, “third” way.
In the second round of the elections both major coalitions stated they would incorporate the “green agenda” into their own plans. Dilma Rousseff was elected by a large political coalition and it is too early to fully understand the broad agenda to be followed by her presidency. The stage is set for the reemergence of the long-term conflict between the so-called “ruralists” (i.e. large farmers and leaders of agribusiness in Brazil) and the MST, the movement of landless peasants, as well as the conflicts between environmentalists and the supporters of accelerated development at the expenses of environmental degradation. Such conflicts tend to be especially violent in Brazil and it is no coincidence that Marina Silva’s regional leadership (in the state of Acre, in the northwest border of Brazil’s Amazon Rain Forest) is usually viewed as a leadership consolidated after the brutal murder of Chico Mendes, her former mentor and the late leader of the Brazilian rubber taper union (http://en.wikipedia.org/wiki/Chico_Mendes).
Brazil ranks nowadays as one of the main forces of agribusiness and the main producer of biofuels (especially sugar cane ethanol), worldwide. The country houses both the largest extensions of pristine forests in the whole world, as well as retaining the unfortunate record of having the fastest pace deforestation rate.
With an expected annual growth of its GDP of 7.5-8% in 2010, Brazil is an emergent partner in the complex and contradictory world agenda on global warming, protection of the environment, and biodiversity.
The world’s environmental agenda remains a big puzzle to be debated in the next rounds of the global diplomacy on the environment and climate changes. There is no consensus either within the US or between the US and its main partners, China and India. Much likely Brazil will have a central role in the global negotiations, depending on its own capacity to establish domestic consensus. Marina Silva is a key term in this global equation.
Global health is closely intertwined with environmental conditions in a broad sense and this interrelationship will undoubtedly become even more entangled in the coming years, with the increase of population, global warming, and scarcity of vital resources such as clean water and non-renewable energy. As a professional working in the field of global health, I see means of sustaining the ‘green agenda’ in Brazil, as globally, both increasingly politically complex and increasingly politically crucial.
Francisco I. Bastos, is a researcher at Fundação Oswaldo Cruz (FIOCRUZ) Rio de Janeiro, Brazil, working with Mailman School faculty to establish a GHI ‘Global Partners Alliance.’ As with all ‘Global Posts’ the views expressed are personal and do not reflect the institutional positions of either FIOCRUZ or Columbia University.
Tuesday, November 23, 2010
Ice, snow and cars: Filing an insurance claim

First: Unless you signed a contract with an insurance company requiring you to take your car only to a specified shop, you can choose where to take it for repair. But the shop still needs to work with the insurer to come to an agreed-upon price. If not, and they still fix the car, you may be responsible for whatever the insurer doesn't pay.
For more details on "diminished value", non-OEM parts, getting a rental car, etc., please see our "How the auto insurance claims process works" page.
If you're in a wreck and it's more than a fender-bender, you might want to see our "What happens if my car gets totaled?" page. From it:
You have the right to payment of the actual cash value of your auto, and to expect a prompt and fair settlement. Don’t be surprised if your “value amount” and the insurer’s “value amount” do not match. Be ready to negotiate with the insurer when this happens.
The page has a lot more information on how insurers establish the cash value of the totaled vehicle, what happens if you can't find a comparable vehicle, and -- we get this question a lot -- what happens if you want to keep your damaged car.
If you have questions or problems with an insurer -- we're the state agency that regulates the insurance industry in Washington state -- give us a call at 1-800-562-6900 or e-mail us at AskMike@oic.wa.gov.
Monday, November 22, 2010
My weekend in Istanbul, and back to home sweet home. By blogger of the month Elizabeth Nowak

So at this point, you’re probably wondering what kind of sorry existence I had in high school. And that would be a pretty fair question. I brought this up not to share with you the incredibly boring details of my past, but because my life in Israel has brought with it a whole new set of borders to explore, and (no offense Canada!) but these ones are a markedly more interesting. As MSIHers, we are in the ideal location to see the world around us, both within Israel and those countries surrounding it. Last week I was honing my procrastination skills and discovered that I could fly to Istanbul for the same price as a ticket from Buffalo to Newark! So I decided to take the weekend off and go to Istanbul.

I had never been to Istanbul before, so I had a lot of catching up to do. I had to make an appearance at all the standard tourist destinations – the Hagia Sophia, the Blue Mosque, and Topkapi Palace. I have to say it was pretty peaceful to spend a few hours gazing up into exquisitely decorated stone tiled domes of these masterpieces. I’m a student, and I can’t really afford tours and whatnot, so I’ve grown accustomed to sneaking around famous landmarks and subtly integrating myself into the other English-speaking tour groups that go by. The nice thing about this method is that you learn a lot of fun facts, and it’s free!

When I got tired, I sought refuge in those places I miss the most from home: Starbucks, and Subway of course. I ended up (much to the chagrin of airport security) bringing a few extra subway subs back to Be’er Sheva with me, just to savor the joy a little longer.

Human traits are distributed along bell curves: You need to know yourself, and HCE can help
Most human traits (e.g., body fat percentage, blood pressure, propensity toward depression) are influenced by our genes; some more than others. The vast majority of traits are also influenced by environmental factors, the “nurture” part of the “nature-nurture” equation. Very few traits are “innate”, such as blood type.
This means that manipulating environmental factors, such as diet and lifestyle, can strongly influence how the traits are finally expressed in humans. But each individual tends to respond differently to diet and lifestyle changes, because each individual is unique in terms of his or her combination of “nature” and “nurture”. Even identical twins are different in that respect.
When plotted, traits that are influenced by our genes are distributed along a bell-shaped curve. For example, a trait like body fat percentage, when measured in a population of 1000 individuals, will yield a distribution of values that will look like a bell-shaped distribution. This type of distribution is also known in statistics as a “normal” distribution.
Why is that?
The additive effect of genes and the bell curve
The reason is purely mathematical. A measurable trait, like body fat percentage, is usually influenced by several genes. (Sometimes individual genes have a very marked effect, as in genes that “switch on or off” other genes.) Those genes appear at random in a population, and their various combinations spread in response to selection pressures. Selection pressures usually cause a narrowing of the bell-shaped curve distributions of traits in populations.
The genes interact with environmental influences, which also have a certain degree of randomness. The result is a massive combined randomness. It is this massive randomness that leads to the bell-curve distribution. The bell curve itself is not random at all, which is a fascinating aspect of this phenomenon. From “chaos” comes “order”. A bell curve is a well-defined curve that is associated with a function, the probability density function.
The underlying mathematical reason for the bell shape is the central limit theorem. The genes are combined in different individuals as combinations of alleles, where each allele is a variation (or mutation) of a gene. An allele set, for genes in different locations of the human DNA, forms a particular allele combination, called a genotype. The alleles combine their effects, usually in an additive fashion, to influence a trait.
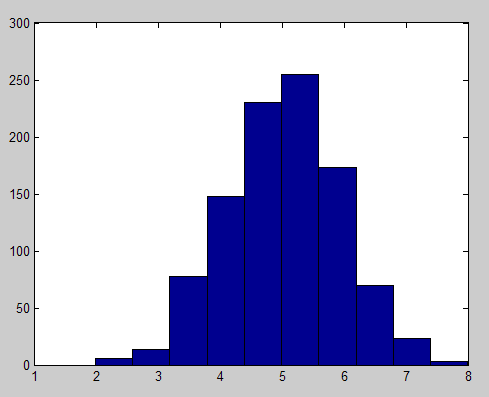
Here is a simple illustration. Let us say one generates 1000 random variables, each storing 10 random values going from 0 to 1. Then the values stored in each of the 1000 random variables are added. This mimics the additive effect of 10 genes with random allele combinations. The result are numbers ranging from 1 to 10, in a population of 1000 individuals; each number is analogous to an allele combination. The resulting histogram, which plots the frequency of each allele combination (or genotype) in the population, is shown on the figure bellow. Each allele configuration will “push for” a particular trait range, making the trait distribution also have the same bell-shaped form.

The bell curve, research studies, and what they mean for you
Studies of the effects of diet and exercise on health variables usually report their results in terms of average responses in a group of participants. Frequently two groups are used, one control and one treatment. For example, in a diet-related study the control group may follow the Standard American Diet, and the treatment group may follow a low carbohydrate diet.
However, you are not the average person; the average person is an abstraction. Research on bell curve distributions tells us that there is about a 68 percentage chance that you will fall within a 1 standard deviation from the average, to the left or the right of the “middle” of the bell curve. Still, even a 0.5 standard deviation above the average is not the average. And, there is approximately a 32 percent chance that you will not be within the larger -1 to 1 standard deviation range. If this is the case, the average results reported may be close to irrelevant for you.
Average results reported in studies are a good starting point for people who are similar to the studies’ participants. But you need to generate your own data, with the goal of “knowing yourself through numbers” by progressively analyzing it. This is akin to building a “numeric diary”. It is not exactly an “N=1” experiment, as some like to say, because you can generate multiple data points (e.g., N=200) on how your body alone responds to diet and lifestyle changes over time.
HealthCorrelator for Excel (HCE)
I think I have finally been able to develop a software tool that can help people do that. I have been using it myself for years, initially as a prototype. You can see the results of my transformation on this post. The challenge for me was to generate a tool that was simple enough to use, and yet powerful enough to give people good insights on what is going on with their body.
The software tool is called HealthCorrelator for Excel (HCE). It runs on Excel, and generates coefficients of association (correlations, which range from -1 to 1) among variables and graphs at the click of a button.
This 5-minute YouTube video shows how the software works in general, and this 10-minute video goes into more detail on how the software can be used to manage a specific health variable. These two videos build on a very small sample dataset, and their focus is on HDL cholesterol management. Nevertheless, the software can be used in the management of just about any health-related variable – e.g., blood glucose, triglycerides, muscle strength, muscle mass, depression episodes etc.
You have to enter data about yourself, and then the software will generate coefficients of association and graphs at the click of a button. As you can see from the videos above, it is very simple. The interpretation of the results is straightforward in most cases, and a bit more complicated in a smaller number of cases. Some results will probably surprise users, and their doctors.
For example, a user who is a patient may be able to show to a doctor that, in the user’s specific case, a diet change influences a particular variable (e.g., triglycerides) much more strongly than a prescription drug or a supplement. More posts will be coming in the future on this blog about these and other related issues.
This means that manipulating environmental factors, such as diet and lifestyle, can strongly influence how the traits are finally expressed in humans. But each individual tends to respond differently to diet and lifestyle changes, because each individual is unique in terms of his or her combination of “nature” and “nurture”. Even identical twins are different in that respect.
When plotted, traits that are influenced by our genes are distributed along a bell-shaped curve. For example, a trait like body fat percentage, when measured in a population of 1000 individuals, will yield a distribution of values that will look like a bell-shaped distribution. This type of distribution is also known in statistics as a “normal” distribution.
Why is that?
The additive effect of genes and the bell curve
The reason is purely mathematical. A measurable trait, like body fat percentage, is usually influenced by several genes. (Sometimes individual genes have a very marked effect, as in genes that “switch on or off” other genes.) Those genes appear at random in a population, and their various combinations spread in response to selection pressures. Selection pressures usually cause a narrowing of the bell-shaped curve distributions of traits in populations.
The genes interact with environmental influences, which also have a certain degree of randomness. The result is a massive combined randomness. It is this massive randomness that leads to the bell-curve distribution. The bell curve itself is not random at all, which is a fascinating aspect of this phenomenon. From “chaos” comes “order”. A bell curve is a well-defined curve that is associated with a function, the probability density function.
The underlying mathematical reason for the bell shape is the central limit theorem. The genes are combined in different individuals as combinations of alleles, where each allele is a variation (or mutation) of a gene. An allele set, for genes in different locations of the human DNA, forms a particular allele combination, called a genotype. The alleles combine their effects, usually in an additive fashion, to influence a trait.
Here is a simple illustration. Let us say one generates 1000 random variables, each storing 10 random values going from 0 to 1. Then the values stored in each of the 1000 random variables are added. This mimics the additive effect of 10 genes with random allele combinations. The result are numbers ranging from 1 to 10, in a population of 1000 individuals; each number is analogous to an allele combination. The resulting histogram, which plots the frequency of each allele combination (or genotype) in the population, is shown on the figure bellow. Each allele configuration will “push for” a particular trait range, making the trait distribution also have the same bell-shaped form.
The bell curve, research studies, and what they mean for you
Studies of the effects of diet and exercise on health variables usually report their results in terms of average responses in a group of participants. Frequently two groups are used, one control and one treatment. For example, in a diet-related study the control group may follow the Standard American Diet, and the treatment group may follow a low carbohydrate diet.
However, you are not the average person; the average person is an abstraction. Research on bell curve distributions tells us that there is about a 68 percentage chance that you will fall within a 1 standard deviation from the average, to the left or the right of the “middle” of the bell curve. Still, even a 0.5 standard deviation above the average is not the average. And, there is approximately a 32 percent chance that you will not be within the larger -1 to 1 standard deviation range. If this is the case, the average results reported may be close to irrelevant for you.
Average results reported in studies are a good starting point for people who are similar to the studies’ participants. But you need to generate your own data, with the goal of “knowing yourself through numbers” by progressively analyzing it. This is akin to building a “numeric diary”. It is not exactly an “N=1” experiment, as some like to say, because you can generate multiple data points (e.g., N=200) on how your body alone responds to diet and lifestyle changes over time.
HealthCorrelator for Excel (HCE)
I think I have finally been able to develop a software tool that can help people do that. I have been using it myself for years, initially as a prototype. You can see the results of my transformation on this post. The challenge for me was to generate a tool that was simple enough to use, and yet powerful enough to give people good insights on what is going on with their body.
The software tool is called HealthCorrelator for Excel (HCE). It runs on Excel, and generates coefficients of association (correlations, which range from -1 to 1) among variables and graphs at the click of a button.
This 5-minute YouTube video shows how the software works in general, and this 10-minute video goes into more detail on how the software can be used to manage a specific health variable. These two videos build on a very small sample dataset, and their focus is on HDL cholesterol management. Nevertheless, the software can be used in the management of just about any health-related variable – e.g., blood glucose, triglycerides, muscle strength, muscle mass, depression episodes etc.
You have to enter data about yourself, and then the software will generate coefficients of association and graphs at the click of a button. As you can see from the videos above, it is very simple. The interpretation of the results is straightforward in most cases, and a bit more complicated in a smaller number of cases. Some results will probably surprise users, and their doctors.
For example, a user who is a patient may be able to show to a doctor that, in the user’s specific case, a diet change influences a particular variable (e.g., triglycerides) much more strongly than a prescription drug or a supplement. More posts will be coming in the future on this blog about these and other related issues.
Sunday, November 21, 2010
Study Favors Chiropractic over Surgical Discectomy for Sciatica

I have had many people avoid surgery with our approach. I often see people who are in severe pain make rash decisions when they are irritable and scared like visiting the emergency room for back pain or immediately undergoing an MRI and taking pills that do not improve function. For Sciatica, see us first. You will get better faster, more safely, with less intervention with care centered on long term resolution of your problem, rather than just the symptom of back pain.
Saturday, November 20, 2010
Glucose Tolerance in Non-industrial Cultures
Background
Glucose is the predominant blood sugar and one of the body's two main fuel sources (the other is fatty acids). Glucose, in one form or another, is also the main form of digestible dietary carbohydrate in nearly all human diets. Starch is made of long chains of glucose molecules, which are rapidly liberated and absorbed during digestion. Sucrose, or table sugar, is made of one glucose and one fructose molecule, which are separated before absorption.
Blood glucose is essential for life, but it can also be damaging if there is too much of it. Therefore, the body tries to keep it within a relatively tight range. Normal fasting glucose is roughly between 70 and 90 mg/dL*, but in the same individual it's usually within about 5 mg/dL on any given day. Sustained glucose above 160 mg/dL or so causes damage to multiple organ systems. Some people would put that number closer to 140 mg/dL.
The amount of glucose contained in a potato far exceeds the amount contained in the blood, so if all that glucose were to enter the blood at once, it would lead to a highly damaging blood glucose level. Fortunately, the body has a hormone designed to keep this from happening: insulin. Insulin tells cells to internalize glucose from the blood, and suppresses glucose release by the liver. It's released by the pancreas in response to eating carbohydrate, and protein to a lesser extent. The amount of insulin released is proportional to the amount of carbohydrate ingested, so that glucose entering the blood is cleared before it can accumulate.
Insulin doesn't clear all the glucose as it enters the bloodstream, however. Some of it does accumulate, leading to a spike in blood glucose. This usually doesn't exceed 130 mg/dL in a truly healthy person, and even if it approaches that level it's only briefly. However, diabetics have reduced insulin signaling, and eating a typical meal can cause their glucose to exceed 300 mg/dL due to reduced insulin action and/or insulin secretion. In affluent nations, this is typically due to type II diabetes, which begins as insulin resistance, a condition in which insulin is actually higher than normal but cells fail to respond to it. The next step is the failure of insulin-secreting beta cells, which is what generally precipitates actual diabetes.
The precursor to diabetes is called glucose intolerance, or pre-diabetes. In someone with glucose intolerance, blood glucose after a typical meal will exceed that of a healthy person, but will not reach the diabetic range (a common definition of diabetes is 200 mg/dL or higher, 2 hours after ingesting 75g of glucose). Glucose tolerance refers to a person's ability to control blood glucose when challenged with dietary glucose, and can be used in some contexts as a useful predictor of diabetes risk and general metabolic health. Doctors use the oral glucose tolerance test (OGTT), which involves drinking 60-100g glucose and measuring blood glucose after one or two hours, to determine glucose tolerance.
Why do we care about glucose tolerance in non-industrial cultures?
One of the problems with modern medical research is that so many people in our culture are metabolically sick that it can be difficult to know if what we consider "normal" is really normal or healthy in the broader sense. Non-industrial cultures allow us to examine what the human metabolism is like in the absence of metabolic disease. I admit this rests on certain assumptions, particularly that these people aren't sick themselves. I don't think all non-industrial cultures are necessarily healthy, but I'm going to stick with those that research has shown have an exceptionally low prevalence of diabetes (by Western standards) and other "diseases of civilization" for the purposes of this post.
Here's the question I really want to answer in this post: do healthy non-industrial cultures with a very high carbohydrate intake have an excellent glucose tolerance, such that their blood glucose doesn't rise to a high level, or are they simply resistant to the damaging effects of high blood glucose?
The data
I'm going to start with an extreme example. In the 1960s, when it was fashionable to study non-industrial cultures, researchers investigated the diet and health of a culture in Tukisenta, in the highlands of Papua New Guinea. The eat practically nothing but sweet potatoes, and their typical daily fare is 94.6 percent carbohydrate. Whether or not you believe that exact number, their diet was clearly extraordinarily high in carbohydrate. They administered 100g OGTTs and measured blood glucose at one hour, which is a very stringent OGTT. They compared the results to those obtained in the 1965 Tecumseh study (US) obtained by the same method. Here's what they found (1):
 Compared to Americans, in Tukisenta they had an extraordinary glucose tolerance at all ages. At one hour, their blood glucose was scarcely above normal fasting values, and glucose tolerance only decreased modestly with age. In contrast, in Americans over 50 years old, the average one-hour value was around 180 mg/dL!
Compared to Americans, in Tukisenta they had an extraordinary glucose tolerance at all ages. At one hour, their blood glucose was scarcely above normal fasting values, and glucose tolerance only decreased modestly with age. In contrast, in Americans over 50 years old, the average one-hour value was around 180 mg/dL!
Now let's take a look at the African Bantu in the Lobaye region of the Central African Republic. The Bantu are a large ethnic group who primarily subsist on a diverse array of starchy foods including grains, beans, plantains and root crops. One hour after a 100g OGTT, their blood glucose was 113 mg/dL, compared to 139 mg/dL in American controls (2). Those numbers are comparable to what investigators found in Tukisenta, and indicate an excellent glucose tolerance in the Bantu.
In South America, different investigators studied a group of native Americans in central Brazil that subsist primarily on cassava (a starchy root crop) and freshwater fish. Average blood glucose one hour after a 100g OGTT was 94 mg/dl, and only 2 out of 106 people tested had a reading over 160 mg/dL (both were older women) (Western Diseases: Their Emergence and Prevention, p. 149). Again, that indicates a phenomenal glucose tolerance by Western standards.
I have to conclude that high-carbohydrate non-industrial cultures probably don't experience damaging high blood glucose levels, because their glucose tolerance is up to the task of shuttling a huge amount of glucose out of the bloodstream before that happens.
Not so fast...
Now let's turn our attention to another study that may throw a wrench in the gears. A while back, I found a paper containing OGTT data for the !Kung San (also called the Bushmen), a hunter-gatherer group living in the Kalahari desert of Africa. I reported in an earlier post that they had a good glucose tolerance. When I revisited the paper recently, I realized I had misread it and in fact, their glucose tolerance was actually pretty poor.
Investigators administered a 50g OGTT, half what the other studies used. At one hour, the San had blood glucose readings of 169 mg/dL, compared to 142 mg/dL in Caucasian controls (3)! I suspect a 100g OGTT would have put them close to the diabetic range.
Wait a minute, these guys are hunter-gatherers living the ancestral lifestyle; aren't they supposed to be super healthy?? First of all, like many hunter-gatherer groups the San are very small people: the men in this study were only 46 kg (101 lbs). The smaller you are, the more a given amount of carbohydrate will raise your blood glucose. Also, while I was mulling this over, I recalled a discussion where non-diabetic people were discussing their 'diabetic' OGTT values while on a low-carbohydrate diet. Apparently, carbohydrate refeeding for a few days generally reverses this and allows a normal OGTT in most people. It turns out this effect has been known for the better part of a century.
So what were the San eating? The study was conducted in October of 1970. The San diet changes seasonally, however their main staple food is the mongongo nut, which is mostly fat and which is available year-round (according to The !Kung San: Men, Women and Work in a Foraging Society). Their carbohydrate intake is generally low by Western standards, and at times of the year it is very low. This varies by the availability of other foods, but they generally don't seem to relish the fibrous starchy root crops that are available in the area, as they mostly eat them when other food is scarce. Jean-Louis Tu has posted a nice analysis of the San diet on BeyondVeg (4). Here's a photo of a San man collecting mongongo nuts from The !Kung San: Men, Women and Work in a Foraging Society:
 What did the authors of the OGTT study have to say about their diet? Acknowledging that prior carbohydrate intake may have played a role in the OGTT results of the San, they made the following remark:
What did the authors of the OGTT study have to say about their diet? Acknowledging that prior carbohydrate intake may have played a role in the OGTT results of the San, they made the following remark:
You can draw your own conclusions, but I think the high OGTT result of the San probably reflect a low habitual carbohydrate intake, and not pre-diabetes. I have a very hard time believing that this culture wasn't able to handle the moderate amount of carbohydrate in their diet effectively, as observers have never described diabetic complications among them.
Putting it all together
This brings me to my hypothesis. I think a healthy human body is extraordinarily flexible in its ability to adapt to a very broad range of carbohydrate intakes, and adjusts glucose tolerance accordingly to maintain carbohydrate handling in a healthy range. In the context of a healthy diet and lifestyle (from birth), I suspect that nearly anyone can adjust to a very high carbohydrate intake without getting dangerous blood glucose spikes. A low carbohydrate intake leads to impaired glucose handling and better fat handling, as one would expect. This can show up as impaired glucose tolerance or even 'diabetes' on an OGTT, but that does not necessarily reflect a pathological state in my opinion.
Every person is different based on lifestyle, diet, personal history and genetics. Not everyone in affluent nations has a good glucose tolerance, and some people will never be able to handle starch effectively under any circumstances. The best way to know how your body reacts to carbohydrate is to test your own post-meal blood glucose using a glucose meter. They are inexpensive and work well. For the most informative result, eat a relatively consistent amount of carbohydrate for a week to allow your body to adapt, then take a glucose measurement 1 and 2 hours after a meal. If you don't eat much carbohydrate, eating a potato might make you think you're diabetic, whereas after a week of adaptation you may find that a large potato does not spike your blood glucose beyond the healthy range.
Exercise is a powerful tool for combating glucose intolerance, as it increases the muscles' demand for glucose, causing them to transport it out of the blood greedily after a meal. Any exercise that depletes muscle glycogen should be effective.
* Assuming a typical carbohydrate intake. Chris Kresser recently argued, based on several studies, that true normal fasting glucose for a person eating a typical amount of carbohydrate is below 83 mg/dL. Low-carbohydrate eating may raise this number, but that doesn't necessarily indicate a pathological change. High-carbohydrate cultures such as the Kitavans, Aymara and New Guineans tend to have fasting values in the low 60s to low 70s. I suspect that a very high carbohydrate intake generally lowers fasting glucose in healthy people. That seems to be the case so far for Chris Voigt, on his diet of 20 potatoes a day. Stay tuned for an interview with Mr. Voigt in early December.
Glucose is the predominant blood sugar and one of the body's two main fuel sources (the other is fatty acids). Glucose, in one form or another, is also the main form of digestible dietary carbohydrate in nearly all human diets. Starch is made of long chains of glucose molecules, which are rapidly liberated and absorbed during digestion. Sucrose, or table sugar, is made of one glucose and one fructose molecule, which are separated before absorption.
Blood glucose is essential for life, but it can also be damaging if there is too much of it. Therefore, the body tries to keep it within a relatively tight range. Normal fasting glucose is roughly between 70 and 90 mg/dL*, but in the same individual it's usually within about 5 mg/dL on any given day. Sustained glucose above 160 mg/dL or so causes damage to multiple organ systems. Some people would put that number closer to 140 mg/dL.
The amount of glucose contained in a potato far exceeds the amount contained in the blood, so if all that glucose were to enter the blood at once, it would lead to a highly damaging blood glucose level. Fortunately, the body has a hormone designed to keep this from happening: insulin. Insulin tells cells to internalize glucose from the blood, and suppresses glucose release by the liver. It's released by the pancreas in response to eating carbohydrate, and protein to a lesser extent. The amount of insulin released is proportional to the amount of carbohydrate ingested, so that glucose entering the blood is cleared before it can accumulate.
Insulin doesn't clear all the glucose as it enters the bloodstream, however. Some of it does accumulate, leading to a spike in blood glucose. This usually doesn't exceed 130 mg/dL in a truly healthy person, and even if it approaches that level it's only briefly. However, diabetics have reduced insulin signaling, and eating a typical meal can cause their glucose to exceed 300 mg/dL due to reduced insulin action and/or insulin secretion. In affluent nations, this is typically due to type II diabetes, which begins as insulin resistance, a condition in which insulin is actually higher than normal but cells fail to respond to it. The next step is the failure of insulin-secreting beta cells, which is what generally precipitates actual diabetes.
The precursor to diabetes is called glucose intolerance, or pre-diabetes. In someone with glucose intolerance, blood glucose after a typical meal will exceed that of a healthy person, but will not reach the diabetic range (a common definition of diabetes is 200 mg/dL or higher, 2 hours after ingesting 75g of glucose). Glucose tolerance refers to a person's ability to control blood glucose when challenged with dietary glucose, and can be used in some contexts as a useful predictor of diabetes risk and general metabolic health. Doctors use the oral glucose tolerance test (OGTT), which involves drinking 60-100g glucose and measuring blood glucose after one or two hours, to determine glucose tolerance.
Why do we care about glucose tolerance in non-industrial cultures?
One of the problems with modern medical research is that so many people in our culture are metabolically sick that it can be difficult to know if what we consider "normal" is really normal or healthy in the broader sense. Non-industrial cultures allow us to examine what the human metabolism is like in the absence of metabolic disease. I admit this rests on certain assumptions, particularly that these people aren't sick themselves. I don't think all non-industrial cultures are necessarily healthy, but I'm going to stick with those that research has shown have an exceptionally low prevalence of diabetes (by Western standards) and other "diseases of civilization" for the purposes of this post.
Here's the question I really want to answer in this post: do healthy non-industrial cultures with a very high carbohydrate intake have an excellent glucose tolerance, such that their blood glucose doesn't rise to a high level, or are they simply resistant to the damaging effects of high blood glucose?
The data
I'm going to start with an extreme example. In the 1960s, when it was fashionable to study non-industrial cultures, researchers investigated the diet and health of a culture in Tukisenta, in the highlands of Papua New Guinea. The eat practically nothing but sweet potatoes, and their typical daily fare is 94.6 percent carbohydrate. Whether or not you believe that exact number, their diet was clearly extraordinarily high in carbohydrate. They administered 100g OGTTs and measured blood glucose at one hour, which is a very stringent OGTT. They compared the results to those obtained in the 1965 Tecumseh study (US) obtained by the same method. Here's what they found (1):
 Compared to Americans, in Tukisenta they had an extraordinary glucose tolerance at all ages. At one hour, their blood glucose was scarcely above normal fasting values, and glucose tolerance only decreased modestly with age. In contrast, in Americans over 50 years old, the average one-hour value was around 180 mg/dL!
Compared to Americans, in Tukisenta they had an extraordinary glucose tolerance at all ages. At one hour, their blood glucose was scarcely above normal fasting values, and glucose tolerance only decreased modestly with age. In contrast, in Americans over 50 years old, the average one-hour value was around 180 mg/dL!Now let's take a look at the African Bantu in the Lobaye region of the Central African Republic. The Bantu are a large ethnic group who primarily subsist on a diverse array of starchy foods including grains, beans, plantains and root crops. One hour after a 100g OGTT, their blood glucose was 113 mg/dL, compared to 139 mg/dL in American controls (2). Those numbers are comparable to what investigators found in Tukisenta, and indicate an excellent glucose tolerance in the Bantu.
In South America, different investigators studied a group of native Americans in central Brazil that subsist primarily on cassava (a starchy root crop) and freshwater fish. Average blood glucose one hour after a 100g OGTT was 94 mg/dl, and only 2 out of 106 people tested had a reading over 160 mg/dL (both were older women) (Western Diseases: Their Emergence and Prevention, p. 149). Again, that indicates a phenomenal glucose tolerance by Western standards.
I have to conclude that high-carbohydrate non-industrial cultures probably don't experience damaging high blood glucose levels, because their glucose tolerance is up to the task of shuttling a huge amount of glucose out of the bloodstream before that happens.
Not so fast...
Now let's turn our attention to another study that may throw a wrench in the gears. A while back, I found a paper containing OGTT data for the !Kung San (also called the Bushmen), a hunter-gatherer group living in the Kalahari desert of Africa. I reported in an earlier post that they had a good glucose tolerance. When I revisited the paper recently, I realized I had misread it and in fact, their glucose tolerance was actually pretty poor.
Investigators administered a 50g OGTT, half what the other studies used. At one hour, the San had blood glucose readings of 169 mg/dL, compared to 142 mg/dL in Caucasian controls (3)! I suspect a 100g OGTT would have put them close to the diabetic range.
Wait a minute, these guys are hunter-gatherers living the ancestral lifestyle; aren't they supposed to be super healthy?? First of all, like many hunter-gatherer groups the San are very small people: the men in this study were only 46 kg (101 lbs). The smaller you are, the more a given amount of carbohydrate will raise your blood glucose. Also, while I was mulling this over, I recalled a discussion where non-diabetic people were discussing their 'diabetic' OGTT values while on a low-carbohydrate diet. Apparently, carbohydrate refeeding for a few days generally reverses this and allows a normal OGTT in most people. It turns out this effect has been known for the better part of a century.
So what were the San eating? The study was conducted in October of 1970. The San diet changes seasonally, however their main staple food is the mongongo nut, which is mostly fat and which is available year-round (according to The !Kung San: Men, Women and Work in a Foraging Society). Their carbohydrate intake is generally low by Western standards, and at times of the year it is very low. This varies by the availability of other foods, but they generally don't seem to relish the fibrous starchy root crops that are available in the area, as they mostly eat them when other food is scarce. Jean-Louis Tu has posted a nice analysis of the San diet on BeyondVeg (4). Here's a photo of a San man collecting mongongo nuts from The !Kung San: Men, Women and Work in a Foraging Society:
 What did the authors of the OGTT study have to say about their diet? Acknowledging that prior carbohydrate intake may have played a role in the OGTT results of the San, they made the following remark:
What did the authors of the OGTT study have to say about their diet? Acknowledging that prior carbohydrate intake may have played a role in the OGTT results of the San, they made the following remark:a retrospective dietary history (M. J. Konner, personal communication, 1971) indicated that the [San], in fact, consumed fairly large amounts of carbohydrate-rich vegetable food during the week before testing.However, the dietary history was not provided, nor has it been published, so we have no way to assess the statement's accuracy or what was meant by "fairly large amounts of carbohydrate-rich vegetable food." Given the fact that the San diet typically ranges from moderately low to very low in carbohydrate, I suspect they were not getting much carbohydrate as a percentage of calories. Looking at the nutritional value of the starchy root foods they typically eat in appendix D of The !Kung San: Men, Women and Work in a Foraging Society, they are fibrous and most contain a low concentration of starch compared to a potato for example. The investigators may have been misled by the volume of these foods eaten, not realizing that they are not as rich in carbohydrate as the starchy root crops they are more familiar with.
You can draw your own conclusions, but I think the high OGTT result of the San probably reflect a low habitual carbohydrate intake, and not pre-diabetes. I have a very hard time believing that this culture wasn't able to handle the moderate amount of carbohydrate in their diet effectively, as observers have never described diabetic complications among them.
Putting it all together
This brings me to my hypothesis. I think a healthy human body is extraordinarily flexible in its ability to adapt to a very broad range of carbohydrate intakes, and adjusts glucose tolerance accordingly to maintain carbohydrate handling in a healthy range. In the context of a healthy diet and lifestyle (from birth), I suspect that nearly anyone can adjust to a very high carbohydrate intake without getting dangerous blood glucose spikes. A low carbohydrate intake leads to impaired glucose handling and better fat handling, as one would expect. This can show up as impaired glucose tolerance or even 'diabetes' on an OGTT, but that does not necessarily reflect a pathological state in my opinion.
Every person is different based on lifestyle, diet, personal history and genetics. Not everyone in affluent nations has a good glucose tolerance, and some people will never be able to handle starch effectively under any circumstances. The best way to know how your body reacts to carbohydrate is to test your own post-meal blood glucose using a glucose meter. They are inexpensive and work well. For the most informative result, eat a relatively consistent amount of carbohydrate for a week to allow your body to adapt, then take a glucose measurement 1 and 2 hours after a meal. If you don't eat much carbohydrate, eating a potato might make you think you're diabetic, whereas after a week of adaptation you may find that a large potato does not spike your blood glucose beyond the healthy range.
Exercise is a powerful tool for combating glucose intolerance, as it increases the muscles' demand for glucose, causing them to transport it out of the blood greedily after a meal. Any exercise that depletes muscle glycogen should be effective.
* Assuming a typical carbohydrate intake. Chris Kresser recently argued, based on several studies, that true normal fasting glucose for a person eating a typical amount of carbohydrate is below 83 mg/dL. Low-carbohydrate eating may raise this number, but that doesn't necessarily indicate a pathological change. High-carbohydrate cultures such as the Kitavans, Aymara and New Guineans tend to have fasting values in the low 60s to low 70s. I suspect that a very high carbohydrate intake generally lowers fasting glucose in healthy people. That seems to be the case so far for Chris Voigt, on his diet of 20 potatoes a day. Stay tuned for an interview with Mr. Voigt in early December.
Friday, November 19, 2010
Issaquah woman sentenced to $300,000 in restitution in insurance fraud case
A King County Superior Court judge today ordered Issaquah's Linda Ann Rose, 67, to pay and forfeit a total of $300,000 in restitution to insurance companies for fraudulent injury claims after a minor accident in a parking lot.
On Nov. 13, 2004, Rose was involved in a parking lot collision in Issaquah. An SUV backed out of a parking stall and struck Rose's rented Ford Mustang. Photos of both vehicles show minimal damage, but Rose claimed that she suffered severe back injuries as a result of the collision.
In 2007, her attorney demanded $656,874 from the SUV owner's insurer, and subsequently filed a personal injury lawsuit in the case.
Investigators from the Washington Insurance Commissioner Mike Kreidler's Special Investigations Unit subsequently concluded that Rose knowingly provided altered medical records to her attorney, and that she had had an injured back "well before" the accident.
Rose entered a modified guilty plea to 3 felony counts of using false claims or proof in an insurance claim.
She was ordered to pay $250,000 to Progressive, $25,000 to Metlife, and to forfeit another $25,000 in a structured settlement from Metlife that had not yet been paid.
On Nov. 13, 2004, Rose was involved in a parking lot collision in Issaquah. An SUV backed out of a parking stall and struck Rose's rented Ford Mustang. Photos of both vehicles show minimal damage, but Rose claimed that she suffered severe back injuries as a result of the collision.
In 2007, her attorney demanded $656,874 from the SUV owner's insurer, and subsequently filed a personal injury lawsuit in the case.
Investigators from the Washington Insurance Commissioner Mike Kreidler's Special Investigations Unit subsequently concluded that Rose knowingly provided altered medical records to her attorney, and that she had had an injured back "well before" the accident.
Rose entered a modified guilty plea to 3 felony counts of using false claims or proof in an insurance claim.
She was ordered to pay $250,000 to Progressive, $25,000 to Metlife, and to forfeit another $25,000 in a structured settlement from Metlife that had not yet been paid.
Thursday, November 18, 2010
Flood coverage: Where to find it -- and what if you can't?

November in the Pacific Northwest generally means rain, and lots of it. (See also December, February, March, April and sometimes May.)
As the rivers swell, we tend to get nervous queries from consumers and businesses about flood insurance. Here are the basics, as well as some special information for businesses in Washington state's Green River Valley.
Does a standard homeowners' insurance cover flooding? No. Many people think it does. It does not.
Where do I get flood coverage? For most consumers and many businesses, the first stop is the National Flood Insurance Program, a federally run program that's been around for decades. But the business coverage maxes out at $500,000 per building and $500,000 for contents, so businesses may need extra coverage as well.
What's it cost? The average federal flood insurance policy costs less than $570 per year.
Am I in a flood zone? Here's a page to search flood maps. You can also get a quick risk estimate by typing your address into the feds' "one-step flood risk profile."
I heard that the federal flood insurance program was suspended. It was, but isn't anymore. The program lapsed several times this year, but Congress in late September reauthorized the program for another year.
Who sells it? Although it's a federally run program, it's sold by many insurance agents. To find a local one who sells it, see the program's agent locator.
And here's the special information for businesses in Washington's Green River Valley, which is in south King County. Last year, businesses in the area reported problems finding additional coverage. To help, we set up a "market assistance plan" that acts as a matchmaker between businesses and insurers. If you live in that area and can't find coverage for your business, the odds are good that the market assistance plan can help you.
For more, please see our flood information page.
As the rivers swell, we tend to get nervous queries from consumers and businesses about flood insurance. Here are the basics, as well as some special information for businesses in Washington state's Green River Valley.
Does a standard homeowners' insurance cover flooding? No. Many people think it does. It does not.
Where do I get flood coverage? For most consumers and many businesses, the first stop is the National Flood Insurance Program, a federally run program that's been around for decades. But the business coverage maxes out at $500,000 per building and $500,000 for contents, so businesses may need extra coverage as well.
What's it cost? The average federal flood insurance policy costs less than $570 per year.
Am I in a flood zone? Here's a page to search flood maps. You can also get a quick risk estimate by typing your address into the feds' "one-step flood risk profile."
I heard that the federal flood insurance program was suspended. It was, but isn't anymore. The program lapsed several times this year, but Congress in late September reauthorized the program for another year.
Who sells it? Although it's a federally run program, it's sold by many insurance agents. To find a local one who sells it, see the program's agent locator.
And here's the special information for businesses in Washington's Green River Valley, which is in south King County. Last year, businesses in the area reported problems finding additional coverage. To help, we set up a "market assistance plan" that acts as a matchmaker between businesses and insurers. If you live in that area and can't find coverage for your business, the odds are good that the market assistance plan can help you.
For more, please see our flood information page.
Restoring comfort and health, one bed at a time

By Rik Ganderton,
RVHS President and CEO
A bed is synonymous with comfort. When you’re sick it can be crucially important to restoring your health.
For whatever reason you find yourself as a patient in the hospital, you will probably be using a bed. The Rouge Valley Centenary Buy a Bed campaign is our challenge to restore comfort and health, one bed at a time as we replace older beds in the hospital.
Replacement beds have been identified as a high-priority need for many departments in the hospital. Beds cost about $5,000 each. Medical beds play a vital role in patient recovery, and in wound and injury prevention. The specialized mattress and frame in a medical bed is built for a lot of use. Special features include patient position monitors and in-bed scales to reduce both patient and caregiver injuries. These elements make them much more expensive than household beds.
The goal of the campaign is to purchase 100 beds during the next two years. This is an achievable goal and we are already well on our way with 45 beds purchased.
I am excited about this campaign, since it is something that everyone is able to easily identify with. The response of the community has been tremendous and we are so thankful for this support. I am also very proud of staff members at Rouge Valley Centenary, who have demonstrated their incredible support of the campaign.
We currently have 67 staff members who have enrolled in payroll deduction and those who have made outright donations. I personally support this campaign, of course.
There are many ways to support the campaign as an individual, or as a group, including sports teams and as colleagues at work. You can help restore comfort and health, one bed at a time. To find out more on this campaign, please visit the RVHS Foundation's Buy-A-Bed web page.
More from our case files...
Having trouble with an insurance company, agent or broker? Give us a call; we can often help. We're the government agency that regulates the insurance industry in Washington state. (If you don't live in Washington, here's an easy map with contact info for our counterparts in your own state.)
In Washington state, we're at 1-800-562-6900 or AskMike@oic.wa.gov. You can now also file a complaint easily online.
Here's a sampling of the sorts of things we help with virtually every day:
In Washington state, we're at 1-800-562-6900 or AskMike@oic.wa.gov. You can now also file a complaint easily online.
Here's a sampling of the sorts of things we help with virtually every day:
- A woman contacted us on behalf of her 75-year-old mother, who had forgotten to pay her long-term care insurance premium due to health issues. The company had cancelled the policy for non-payment. After multiple attempts to have the policy reinstated, the daughter sought our help. The policy was reinstated.
- A company that had sold an illegal discount health plan here agreed to pay a consumer $3,825.
- A widow whose annuity request had been delayed complained to us. We contacted the company, which honored the request, sending her a check for more than $250,000.
Wednesday, November 17, 2010

{kind=link}
Job openings
We have a couple of job openings:
We're looking for an administrative assistant 4 for a limited-duration position funded by federal grant dollars related to health care reform. This person will perform "a wide range of complex administrative duties related to planning and implementation of organizational change, grant management and program support functions." The job duties include compiling statistical information and preparing written reports for executive managers and the grant funding agency. The position is funded by federal grants through November 2011.
Here's the link to the job posting, but if you want to apply, please do it quickly. Applications are due by 4:59 p.m. this Friday.
We're also looking for a financial examiner 2 to work in our Seattle office. This person will plan and conduct financial examinations of insurance companies and other regulated entities. From the job listing:
We're a small state agency -- we have a total of about 200 workers between our Tumwater, Olympia, Seattle and Spokane offices -- that regulates the insurance industry in Washington state. We have a pretty broad consumer-protection mission. We:
We're looking for an administrative assistant 4 for a limited-duration position funded by federal grant dollars related to health care reform. This person will perform "a wide range of complex administrative duties related to planning and implementation of organizational change, grant management and program support functions." The job duties include compiling statistical information and preparing written reports for executive managers and the grant funding agency. The position is funded by federal grants through November 2011.
Here's the link to the job posting, but if you want to apply, please do it quickly. Applications are due by 4:59 p.m. this Friday.
We're also looking for a financial examiner 2 to work in our Seattle office. This person will plan and conduct financial examinations of insurance companies and other regulated entities. From the job listing:
This position works with Financial Analysts (certified public accountants, certified financial examiners, and accredited financial examiners), attorneys, and other regulators on a state, national, and international level. This position examines, audits, and verifies specific groups of insurance companies, including bonds and stocks, mortgage loans, real estate, policy loans, premium notes, collateral loans, policy reserves, and capital stock.For qualifications, pay, and application information, please see this job posting. The deadline for applications is 5 p.m. on Dec. 3.
We're a small state agency -- we have a total of about 200 workers between our Tumwater, Olympia, Seattle and Spokane offices -- that regulates the insurance industry in Washington state. We have a pretty broad consumer-protection mission. We:
- monitor insurers' finances to make sure they can make good on their promises to policyholders.
- license tens of thousands of agents and brokers, and investigates complaints about them.
- scrutinize rate hike requests and makes sure that policies comply with the law.
- go after scams, both from unlicensed insurance companies and by people trying to defraud insurers.
How Washingtonians can file an insurance complaint online

We've launched a new "online consumer complaint center" this week, and we think we're the first state insurance department in the country to offer this kind of service.
The system lets Washington state consumers file complaints against insurers using a new interactive and password-protected web tool.
The idea is to make it more convenient and efficient for consumers to file a complaint with our office. We help with thousands of complaints, but until now, the process has relied on people mailing documents back and forth. We think this will be faster and easier.
What sorts of complaints? They often involve what insurers are covering -- or not covering . We often get calls from drivers whose cars are totalled, and who are unhappy about the payment offered for their vehicle. We try to help with complaints about delayed payments, policies being canceled, getting companies to reopen a claim or negotiate on payment, etc.
At our site, Washington state residents can file a secure complaint online, track its status 24/7, upload documents/photos/etc. related to the case, add comments, and view, print and save information about the case.
Not a Washington state resident? Here's a map with contact info for your own state's insurance department.
Breast Cancer: Risk Factors Rarely Mentioned

Annemarie Colbin was one of my favorite guest speakers while attending the Institute for Integrative Nutrition. This information was in her e-newsletter last month (October) for cancer awareness month and I thought it was worth sharing.
Breast Cancer: Risk Factors Rarely Mentioned
By Annemarie Colbin, Ph.D.
We have been told that women have a 1-in-8 lifetime risk of getting breast cancer. To the statistically naive, that appears to mean that one in eight women will be stricken at some point in her life. Scary? Well, it's not that simple. Here is a more accurate description of the statistical chances of contracting breast cancer according to ages:
WOMAN'S BREAST CANCER STATISTICS:
At age 20: 1 in 2500
At age 30: 1 in 233
At age 40: 1 in 63
At age 50: 1 in 41
At age 60: 1 in 28
At age 70: 1 in 24
At age 80: 1 in 16
At age 90: 1 in 8
Looks quite different, doesn't it? The risk increases with age, and 1-in-8 figure applies only if you live to be 95. That gives us some time. As Mark Twain once said, "there are lies, damn lies, and statistics."
Let's now look at the variables that affect breast health, and I'm going to focus on some of the lesser discussed ones:
Number of children. Having children is protective against breast cancer; in fact, the more children, the higher the protection. One study found that women who have seven or more children had a 47% less chance of developing the disease than women who'd had only one child. This probably has to do with the fact that with more children a woman has less menstrual periods, thus less up- and-down estrogen fluctuations.
Breast-feeding. The function of a woman's breasts is to secrete milk for her newborn, especially if she has actually been pregnant. Pregnancy initiates changes in the breasts, preparing them for lactation. If that process is interrupted or not allowed to proceed, through miscarriage or by bottle-feeding, the body has to deal with the aftermath. Plugged milk ducts can result in lumps; while these would start off generally benign, over time, with other risk factors, they could become cancerous. In fact, all breast cancers arise in the milk ducts. Short breast-feeding has not shown any protective effect; what counts is the accumulated time of breast-feeding during the whole of a woman's life. In the study mentioned, women with a lifetime total of 25 or more months of breast-feeding had a 33% lower risk for contracting breast cancer as compared to women with natural children who had never breast-fed. I will assume that suppressing lactation with drugs can also have serious adverse effects on the breast.
Environmental causes. There are a number of external factors that may affect a woman's hormonal health. The main ones are pesticides, particularly organochlorides, and living near nuclear reactors. Many petroleum-based pesticides imitate the form of estrogen, and confuse the body into accepting them into their cells. They are sprayed on fruits, vegetables, and animal feed; when these are consumed, the pesticides then are stored in human and animal fat, which, according to Connecticut nutritionist Phyllis Herman, may explain the link between a high animal fat diet and breast cancer. A 1990 study in Israel found a strong link: between 1976 and 1986, the rate of breast cancer declined 20% after a number of organochlorine-type pesticides were banned. Industrial countries where breast cancer mortality declined between 1971 and 1986 had no large commercial nuclear reactors operating within or near their borders; the other 12 industrial powers did, and breast cancer rose in them all. It is thought that low-level radioactive contamination enters the groundwater, affecting produce, and is also carried downwind, affecting both animals and people. These environmental reasons are perhaps why breast cancer mortality rates for Long Island went up 39% between 1970 and 1989.
Use of antiperspirants. Here is a very intriguing thought. Kerri Bodner, publisher of the excellent Women's Health Letter, points out that 50% of breast cancer tumors appear on the upper quadrant of the breast closest to the underarm. Antiperspirants are strong chemicals, usually containing aluminum, which prevent sweating. Now sweating is a way for the body to eliminate toxins and unwanted materials with the help of the lymphatic system. Preventing this activity is, in Bodner's words, "like damming up a river." Sweat backs up into the lymphatic ducts, and the toxins become trapped in the under-arm lymphatic area. The fatty breast tissue allows for efficient storage of these unwanted toxins. Breast cancer often involves the lymph nodes. Could there be a connection?
Tight and underwire bras. I remember reading an article that pointed out an increased risk of breast cancer for women who used tight bras, particularly if they wore them for more than 12 hours. Tight bras also interfere with breathing, which may in turn cause oxygen deprivation in the cells. I personally have great antipathy to underwire bras: the metal in them crosses the body's acupuncture meridians, and so can block the normal flow of Chi which in turn can cause stagnation and disease. Why do women through the ages feel they have to mold themselves into some shape dictated by social whim?
The use of oral contraceptives. Numerous studies have shown the direct correlation between hormone-based drugs and female cancers. The latest is a study published in The Lancet, the prestigious British medical journal, on the effects of The Pill on 150,000 women. It found that all users face an increased risk, even 10 years after stopping. Women on the Pill had a 25% higher risk of contracting breast cancer. A study in 1994 had found that women who started on the Pill before the age of 20 had a 3 ½ times higher risk, while 97% of the women who got cancer before the age of 36 had used birth control pills at one time or another of their lives. Note that this does NOT mean that 97% of the women who took birth control pills got cancer; it's the other way around. Obviously there are other variables triggering the disease.
Diet. Fat is suspect, but studies give conflicting results and the issue is not conclusive. It is often mentioned that Japanese women eating their traditional low-fat diets have little if any breast cancer, but when they come to the US they soon catch up. I maintain that fat is not the issue: milk products are. The Japanese diet has no milk products, but now that they are picking up "Western" dietary habits, their use of these products is going up and so is their breast cancer. The highest rates of the disease are in Northern Europe (Finland, Sweden, Holland), the UK, the US, and Canada -- all countries where cow's milk is a major food. Frequent consumption of whole milk has been found to be a risk factor in cancers of the lung, bladder, breast, and cervix; even more interesting, breast cancer patients were found to have twice as high a consumption of Vitamin D (usually added to milk) as cancer-free controls.
What foods protect against cancer? Cruciferous vegetables clearly do: cabbage, broccoli, cauliflower, Brussels sprouts, kale, kohlrabi. Soybeans have also been developing a good reputation as anti-cancer foods. Miso and tofu are excellent additions to your diet.
Here is a simple recipe:
MISO - TOFU SPREAD
½ block soft tofu, steamed for 3 minutes and cooled (about 5 oz)
1 tablespoon brown rice or barley miso
1 tablespoon flaxseed or extra virgin olive oil
2 tablespoons grated onion
Mash all the ingredients together in a bowl, and serve on wholegrain bread or rye crackers.
About Annemarie Colbin:
Annemarie Colbin, Ph.D,
founded the Natural Gourmet in 1977 and is currently its CEO. She has been called a "maverick nutritional theorist", and is an internationally recognized health educator, author, consultant and speaker, specializing in food and its effects on health. She is the author of Food and Healing, which has been translated into six languages, The Natural Gourmet (both from Ballentine Books) and her latest book, The Whole-Food Guide to Strong Bones (New Harbinger Publications, 2009).
Dr. Colbin writes a regular column for New York Spirit magazine, lectures widely, and does personal nutritional counseling for individuals and families. She has won awards for her teaching, writing, educational work and business activities. Her personal website here.
Keep it Fresh!
- Lauren
Request for proposals re: insurance rate review
We're looking for proposals from firms interesting in participating in a project to improve our review of health insurance rates and to increase public transparency for how health insurance premiums are determined.
Interested in bidding? The full request for proposals document is here.
The estimated time period for the contract is Feb. 16, 2011 to Sept. 30, 2011. We reserve the right to extend it for up to three one-year periods; see the RFP for details. It includs the scope of work, evaluation procedures, minimum qualifications, etc.
All proposals are due no later than 5 p.m. PST on Dec. 27, 2010.
For additional details, see also our general RFP page, and see this news release, which contains more information about the federal grant that's helping pay for the project.
Interested in bidding? The full request for proposals document is here.
The estimated time period for the contract is Feb. 16, 2011 to Sept. 30, 2011. We reserve the right to extend it for up to three one-year periods; see the RFP for details. It includs the scope of work, evaluation procedures, minimum qualifications, etc.
All proposals are due no later than 5 p.m. PST on Dec. 27, 2010.
For additional details, see also our general RFP page, and see this news release, which contains more information about the federal grant that's helping pay for the project.
Tuesday, November 16, 2010
Impressions from the Wise Traditions Conference
I spent last weekend at the Weston A. Price Foundation Wise Traditions conference in King of Prussia, PA. Here are some highlights:
Spending time with several people in the diet-health community who I’ve been wanting to meet in person, including Chris Masterjohn, Melissa McEwen and John Durant. John and Melissa are the public face of the New York city paleo movement. The four of us spent most of the weekend together tossing around ideas and making merry. I’ve been corresponding with Chris quite a bit lately and we’ve been thinking through some important diet-health questions together. He is brimming with good ideas. I also got to meet Sally Fallon Morell, the founder and president of the WAPF.
Attending talks. The highlight was Chris Masterjohn’s talk “Heart Disease and Molecular Degeneration: the New Paradigm”, in which he described his compelling theory on oxidative damage and cardiovascular disease, among other things. You can read some of his earlier ideas on the subject here. Another talk I really enjoyed was by Anore Jones, who lived with an isolated Inuit group in Alaska for 23 years and ate a mostly traditional hunter-gatherer diet. The food and preparation techniques they used were really interesting, including various techniques for extracting fats and preserving meats, berries and greens by fermentation. Jones has published books on the subject that I suspect would be very interesting, including Nauriat Niginaqtuat, Plants that We Eat, and Iqaluich Niginaqtuat, Fish that We Eat. The latter is freely available on the web here.
I attended a speech by Joel Salatin, the prolific Virginia farmer, writer and agricultural innovator, which was fun. I enjoyed Sally Fallon Morell’s talk on US school lunches and the politics surrounding them. I also attended a talk on food politics by Judith McGeary, a farmer, attorney and and activist, in which she described the reasons to oppose or modify senate bill 510. The gist is that it will be disproportionately hard on small farmers who are already disfavored by current regulations, making high quality food more difficult to obtain, more expensive or even illegal. It’s designed to improve food safety by targeting sources of food-borne pathogens, but how much are we going to have to cripple national food quality and farmer livelihood to achieve this, and will it even be effective? I don’t remember which speaker said this quote, and I’m paraphrasing, but it stuck with me: “I just want to be able to eat the same food my grandmother ate.” In 2010, that’s already difficult to achieve. Will it be impossible in 2030?
Giving my own talk. I thought it went well, although attendance was not as high as I had hoped. The talk was titled “Kakana Dina: Diet and Health in the Pacific Islands”, and in it I examined the relationship between diet and health in Pacific island cultures with different diets and at various stages of modernization. I’ve covered some of this material on my blog, in my posts on Kitava, Tokelau and sweet potato eating cultures in New Guinea, but other material was new and I went into greater detail on food habits and preparation methods. I also dug up a number of historical photos dating back as far as the 1870s.
The food. All the meat was pasture-raised, organic and locally sourced if possible. There was raw pasture-raised cheese, milk and butter. There was wild-caught fish. There were many fermented foods, including sauerkraut, kombucha and sourdough bread. I was really impressed that they were able to put this together for an entire conference.
The vendors. There was an assortment of wholesome and traditional foods, particularly fermented foods, quality dairy and pastured meats. There was an entire farmer’s market on-site on Saturday, with a number of Mennonite vendors selling traditional foods. I bought a bottle of beet kvass, a traditional Russian drink used for flavor and medicine, which was much better than the beet kvass I’ve made myself in the past. Beets are a remarkable food, in part due to their high nitrate content—beet juice has been shown to reduce high blood pressure substantially, possibly by increasing the important signaling molecule nitric oxide. I got to meet Sandeep Agarwal and his family, owners of the company Pure Indian Foods, which domestically produces top-quality pasture-fed ghee (Indian-style clarified butter). They now make tasty spiced ghee in addition to the plain flavor. Sandeep and family donated ghee for the big dinner on Saturday, which was used to cook delicious wild-caught salmon steaks donated by Vital Choice.
There were some elements of the conference that were not to my taste. But overall I’m glad I was able to go, meet some interesting people, give my talk and learn a thing or two.
Subscribe to:
Comments (Atom)